There is a wide spectrum of pigmented lesions which present an oral mucosa or skin in the head and neck area. In the oral cavity some of the pigmented lesions are physiologic, but most are considered pathologic. The clinical features of benign and malignant lesions of oral mucosa are, in most instances, virtually indistinguishable. This makes it impossible for the clinician to arrive at a definitive diagnosis without biopsy and histopathologic examination of such lesions.
Some of the pigmented lesions of oral mucosa and facial skin include:
1. Normal physiologic pigmentation
2. Ephelis
3. Lentigo
4. Melanotic macule
5. Melanoacanthoma
6. Nevi
7. Melanoma
8. Pigmentation secondary to pregnancy
9. Pigmentation secondary to some other pathologic condition
Melanocytic Lesions
1. Normal physiologic intra-oral pigmentation
- observed in all racial groups, but to varying degrees
- characterized by symmetry
- virtually always asymptomatic
- most common sites involved are gingiva and buccal mucosa
- melanin pigment incontinence (spillage from epithelium into underlying
connective tissue)
2. Ephelis

- Freckle
- Usually limited to sun exposed facial skin, but may involve lip mucosa.
- Normal number of melanocytes in relation to keratinocytes.
- Melanocytes have increased number of melanosomes in their cytoplasm hence more melanin is produced.
- Physiologic response to protect epithelium from uv radiation in sunlight
- Normal thickness of epithelium, no increase in keratinocyte population
3. Lentigo

- 3 variants: simple, solar, and maligna
- Simple lentigo features
a) no predilection for sun exposed skin
b) flat surface and uniform brown color
c) relative increased number of melanocytes as epithelial layer is
thicker (elongated rete ridges)
- solar lentigo features
a) sun exposed skin
b) middle age or elderly population
c) multiple lesions of uniform brown color
- lentigo maligna features
a) histopathologically atypical melanocytes limited to epithelium
b) melanoma in situ or precancerous melanosis
c) lacks invasion warranting diagnosis of lentigo maligna melanoma
4. Melanotic macule

- flat (macular) surface
- well circumscribed border
- focal concentration of normal melanocytes in basal layer of epithelium
5. Melanoacanthoma

- facial skin and oral mucosal lesions significantly different
- facial skin lesion
a) elderly
b) caucasians
c) slow growth
- oral mucosa lesion
a) young adults
b) blacks
c) rapid growth to large size (4 cm in 4 weeks)
d) oral lesion can frequently be associated with irritation or trauma
e) increased number of both normal appearing melanocytes and
keratinocytes, with melanocytes migrating through all layers of
epithelium which is also a feature of melanomas
f) potential for misdiagnosis and radical overtreatment
g) resolves following biopsy or removal of irritation
6. Nevi
- congenital and acquired variants
- may be flat, slightly elevated papillary, pedunculated (on stalk) or nodular
(dome shaped)
- usually well circumscribed
- pigmented or amelanotic (non-pigmented)
- congenital nevus

a) incidence 1% live births
b) usually larger than acquired nevi (>1.5 cm diameter)
c) considered giant nevus if >20 cm
d) often has shape of garment
e) can exhibit hair growth as well as pigmentation
f) malignant transformation 1%, if giant nevus 6-12%
g) excise if possible
- intradermal nevus

a) most common oral variant (55%)
b) can have any surface morphology
c) nests and sheets of nevus cells within supporting connective tissue
(dermis) without epithelial melanocyte proliferation
d) neural nevus is a type of intradermal nevus in which nevus cells
assume a spindle shape and this lesion can be misdiagnosed by
pathologists as a neurofibroma
- junctional nevus

a) usually presents as a flat (macular) lesion which relates to lack of
connective tissue involvement
b) nodule formation observed in intradermal or compound nevi or when
flat surface melanoma in situ invades connective tissue
c) melanocytes in basal layer of epithelium aggregate into clusters or
nests called theques
- compound nevus

a) combination of intradermal and junctional nevus features, that is
nevus cells observed as islands in dermis and forming intra-epithelial
theques
b) some believe junctional activity decreases as lesion matures
- blue nevus

a) second most common oral variant (35%)
b) characteristic blue-black color
c) common form <1 cm in diameter, cellular form >1 cm
d) melanocytes usually appear as pigmented spindle cells in deeper
connective tissue having failed to migrate to epithelium from neural
crest during embryogenesis
e) extremely rare malignant blue nevus reported
- mongolian spot

a) bluish discoloration clinically resembling bruise at base of spinal cord
b) more common in black and asian population
c) presents at or near birth, resolves by early childhood in blacks, may
persist into adulthood in asians
d) results from delayed disappearance of dermal melanocytes
- nevus of Ota

a) speckled blue-black pigmentation following distribution of trigeminal
nerve branches 1 and 2
b) may have synchronous skin and intra-oral lesions
- nevus of Ito

a) associated with nevus of Ota
b) follows distribution of supraclavicular, scapular and deltoid nerves
- epithelioid and spindle cell (Spitz) nevus
a) first reported in 1948 by Spitz as benign juvenile melanoma
b) pink skin nodule
c) clinically resembles pyogenic granuloma
d) most common in children but 25% are reported in patients over age 30
e) epithelioid and spindle shaped cells, clefting at the junction of
epithelium and supporting connective tissue and fibrosis
- halo nevus

a) clinically pigment nevus of any variant surrounded by a zone of
depigmented epithelium
b) correlates with a prominent lymphocyte response surround nevus on
histopathologic examination
- dysplastic nevus

a) first reported as lesion of BK mole syndrome describing familial
tendency of patients with multiple pigmented lesions to develop
melanoma
b) subsequently patients with single isolated lesions with this histo-
pathologic presentation failed to develop melanoma
c) large size (>5 cm diameter), ill defined border
d) irregular pigmentation, multinodular
e) clinically similar to superficial spreading melanoma
f) compound nevus with elongation of epithelial rete ridges
g) some consider a borderline or premalignant lesion
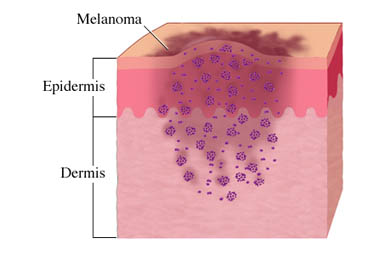
7. Melanoma

- background information
a) incidence (US): 14/100,000 males and 10/10,000 females
b) 1995 ACS statistics: 34,100 new cases
c) 1995 ACS statistics: 7,200 deaths
d) predominantly caucasians (13:1)
e) incidence predicted to increase due to sun exposure and loss of
protective effect afforded by ozone layer
UVB (290-320 mm) being most carcinogenic
f) increased risk with fair complexion, tendency to sunburn rather
than tan, history of blistering sunburn in childhood
g) family history of melanoma increases risk eightfold
h) as incidence increases, so does improved prognosis
i) in oral cavity, metastatic melanoma significantly most likely than
primary disease
- signs and symptoms
a) change in color or size of a pigmented lesion
b) satellite areas of pigmentation
c) bleeding or ulceration of lesion
d) inflammation surrounding lesion
e) pain and/or itching of lesion
- classification of primary skin melanoma
a) lentigo maligna melanoma
* acral lentiginous melanoma
b) superficial spreading melanoma
c) nodular melanoma
- growth phases
a) horizontal (peripheral expansion) and vertical (downward invasion)
b) extent and duration of horizontal growth phase differs for each
variant of melanoma
c) prognosis after invasion similar for all variants
- lentigo maligna melanoma
a) terminology
* lentigo maligna: melanoma in situ
* lentigo maligna melanoma: invasive melanoma
b) large size (4-6 cm average diameter)
c) flat surface
d) long horizontal growth phase averaging 10-15 years
e) earliest expected vertical growth phase is 2-4 after onset
- acral lentiginous melanoma
a) observed on oral or genital mucosa and the extremities
b) essentially an aggressive form of lentigo maligna melanoma
c) prominent dendritic processes similar to melanoacanthoma
d) vertical growth phase lacks clinical warning sign of nodularity
from a previously flat lesion
e) exhibits multifocal invasion and widespread dissemination
- superficial spreading melanoma
a) most common skin variant (70%)
b) predominant sites
*males: head, neck and trunk
*females: back of legs
c) typically smaller size than lentigo maligna melanoma with average
diameter of 2 cm
d) slightly elevated
e) shorter duration for horizontal growth phase before invasion
downwards, averaging 1 year from onset
- nodular melanoma
a) rapid increase in size
b) very short horizontal growth phase before invasion, measured in
weeks
c) worst prognosis
- primary oral melanoma
a) uncommon, 1% of all primary melanoma, oral cavity melanoma much
more likely to represent metastasis
b) most common sites: maxillary alveolar ridge and palate (80%)
c) male predominance (2:1)
d) middle age (average 55 years)
e) prognosis grave, 5 year survival < 10%
- classification of oral melanoma
a) acral lentiginous (most common)
b) superficial spreading
c) nodular
- biopsy considerations
a) melanocytic lesions are clinically indistinguishable making all, at
least potentially malignant melanoma; therefore, all require biopsy
and histopathologic examination to establish a definitive diagnosis
b) total excision as a first procedure is preferred
c) suggest referral to surgeon who will perform definitive surgery
rather than perform incisional biopsy with referral following
histopathologic interpretation
d) cervical lymph nodes following incisional biopsy may be clinically
enlarged and suggest metastasis, mandating surgical exploration of
the neck
e) if lesion is too large to excise for biopsy, sample from darkest or
most nodular area
- treatment considerations
a) surgical
* wide to radical tumor excision
* therapeutic regional lymph node dissection for obvious
metastasis, elective dissection in search of occult metastasis
* tumor invasion < 0.75 mm predictably non metastatic
* tumor invasion > 1.50 mm worrisome for occult metastasis
* tumor invasion > 3.59 mm generally too late to prevent
metastasis
* 40% primary oral melanoma have metastasized when patient
initially presents
* distant metastasis associated more with uncontrolled disease
at primary site (i.e.: inadequate initial surgery) than regional
nodal metastasis
* average interval to relapse following surgery 8.5 months
b) radiation therapy
* high dose fractions 2400cGy over 21days had 53% partial and
30% complete remission in one study
* fast neutrons vis a vis orthovoltage
* hyperthermia enhancement
* radiosensitizers: boron (absorbs fast neutrons) combined with
chlorpromazine (affinity for melanoma cells)
c) adjunctive chemotherapy
* DTIC
* cisplatin
* nitrosurea
* tamoxifen
d) immunotherapy
* bacillus calmette-guerin (BCG) stimulation of immune system
effective in early disease but has little positive effect (7%) once
melanoma has metastasized
e) biologic response modifiers
* high dose interleuken II stimulates tumor infiltrating
lymphocytes (TIL) to attack melanoma cells
* monoclonal tumor antibody vaccine
- prognostic factors
a) histopathologic factors and clinical stage (extent) both considered
important in determining patient outcome
b) tumor thickness (volume) and depth of invasion are most important
histopathologic factors in determining patient outcome
c) Clark method measures tumor invasion utilizing anatomic layers
d) Breslow method measures tumor invasion in mm utilizing calibrated
microscope
e) mitotic index of >2 per 10 microscopic high power fields reduces 5
year survival 20%, all other factors being equal
f) ulceration due to ischemia (tumor growth outrunning its blood supply)
associated with reduced survival
g) increased patient age reduces prognosis
h) females have slightly better survival rate (7%) than men, all other
factors being equal
- survival estimates based on depth of invasion
a) Clark method of determining depth of invasion
Clark 1 melanoma in situ (no invasion)
Clark 2 tumor in papillary dermis
Clark 3 tumor to junction of papillary and reticular dermis
Clark 4 tumor in reticular dermis
Clark 5 tumor in subcutaneous tissues
Level 5 Year 10 Year
1 100% 96%
2 92% 96%
3 65% 90%
4 54% 67%
5 48% 26%
b) Breslow method of determining depth of invasion
Breslow 1 0.00 - 0.75 mm invasion
Breslow 2 0.76 - 1.69 mm invasion
Breslow 3 1.70 - 3.50 mm invasion
Breslow 4 3.60 mm or greater invasion
Level 5 Year 10 Year
1 99% 98%
2 94% 89%
3 81% 67%
4 49% 43%
- survival estimates based on staging
a) TNM method
stage 1 lesions without metastasis
stage 2 lesions with metastasis to only 1 regional
lymph node
stage 3 disseminated metastasis
TNM 5 Year 10 Year
stage 1 89% 81%
no recurrence 88%
local recurrence 42%
stage 2 61% 47%
1 node 45%
2 nodes 28%
3 nodes 9%
stage 3 2% 0%
- metastatic melanoma to the oral cavity based on 800 cases NIH study
a) 3% of skin melanoma metastasize to oral cavity
b) primary is usually in the head or neck area
c) male predilection (3:2)
d) average age 40 years
e) average interval between primary and metastatic lesion is 4.2 years
f) most common metastatic sites: tongue, cheek, parotid gland, alveolus
g) metastatic melanoma to parotid gland lymph nodes commonly from
primary in scalp
h) metastatic melanoma may be non-pigmented
i) symptoms may include tooth mobility, non-healing extraction sites
and tumor expressing from extraction socket
8. Pigmentation secondary to pregnancy

- probable association with increased ACTH during pregnancy
- ACTH mimics chemical structure of HSH (melanin stimulating hormone)
- chloasma: (pregnancy mask) irregular, flat areas of pigmentation on facial
skin of women during 2nd and 3rd trimesters
- melasma: circumoral pigmentation at vermilion border may also been
observed in women taking birth control pills
9. Pigmentation secondary to Acanthosis Nigricans

- thickened skin and oral mucosa
- seen in childhood as a benign process
- cutaneous marker for internal malignancy in adults, chiefly gastrointestinal
carcinoma
- oral lesion may exhibit papillary surface and/or pigmentation
10. Pigmentation secondary to Peutz-Jegher syndrome

- syndrome characterized by circumoral pigmentation and multiple intestinal
polyps
- polyps can involute (intusseption) and obstruct causing surgical emergency
- malignant transformation very low in comparison to polyposis of Gardner’s
syndrome
11. Pigmentation secondary to neurofibromatosis

- multiple neurofibroma of skin and oral mucosa
- multiple areas of skin pigmentation known as café au lait spots (coffee with
cream color)
- low potential (2%) for malignant transformation of benign neurofibroma
into neurogenic sarcoma
- Von Recklinghausen’s disease of skin
12. Pigmentation secondary to chronic adrenocortical insufficiency
- primary form of condition due to autoimmune destruction of adrenal cortex
- pituitary gland continues to secrete ACTH as biofeedback mechanism to
terminate process cannot be performed by affected adrenal cortex
- ACTH stereochemically similar to MSH (melanin stimulating hormone)
- excess ACTH causes bronzing of skin and oral pigmentation
- Addison’s disease
13. Pigmentation secondary to malignant tumors
- oat cell carcinoma of the lung produce ectopic ACTH which may elicit oral
pigmentation
- generalized melanosis of skin observed in patients with disseminated
metastatic melanoma
14. Pigmentation secondary to vitamin deficiency
- pellegra (niacin deficiency) can produce a skin rash and hyperpigmentation
of exposed facial skin
- oral lesion is an enlarged beefy red tongue
15. Pigmentation secondary to therapeutic drugs
- oral contraceptives
- chloroquinine used as anti-malarial and control of lupus erythematosus
- tetracycline administered over long duration can alter oral microflora and
enhance conditions for development of brown or black hairy tongue
- thorazine used in the treatment of psychosis
- minocine antibiotic causes blue gray discoloration of bone
- quinibrine used as anti-helminthic causes yellow discoloration of skin and
oral mucous clinically similar to jaundice
- over the counter preparations such as laxatives taken in excess can cause
pigment deposition in mucosa
16. Pigmentation secondary to Albright’s syndrome
- polystotic (multiple site) fibrous dysplasia
- café au lait colored skin and oral mucosal pigmentation
- in females, precocious puberty
17. Neonatal pigmentation secondary to tumor
- neuroectodermal tumor of infancy
a) most common site is anterior maxilla
b) melanin pigmentation deposition in mucosa
c) radiographic presentation is well circumscribed radiolucency
surrounding developing tooth
d) vanillymandelic acid (VMA) from metabolism of excess
catecholamines (epinephrine and norepinephrine) found in urine
18. Pigmentation secondary to systemic intoxication (poisoning) by heavy metals
- lead poisoning
a) lead sulfate deposition in gingival sulcus (Burton’s line)
b) excessive salivation (ptyalism)
c) peripheral neuropathy and learning defects associated
d) treat with chelating agents
- mercury
- bismuth
- arsenic
- gold
19. Pigmentation secondary to foreign body implantation
- amalgam tattoo
a) most common sites are gingiva and buccal mucosa
b) radiographic discovery may allow clinical correlation precluding
necessity for biopsy and histopathologic examination
c) focal argyrosis
- graphite
a) most common sites are palate, floor of mouth and lip
b) history of accidental puncture by pencil may be recounted
20. Pathologic conditions which mimic melanocytic lesions
- hematoma
a) secondary to trauma
b) recurrent lesions suggest abuse
- hemangioma
a) most common mesenchymal tumor in childhood
b) dioscopy test positive
c) treat by a variety of modalities
- varix
a) vascular anomaly often with thrombus
b) essentially a varicose vein
- Kaposi sarcoma
a) usually red to purple in color but may exhibit a brown hue
b) malignant blood vessel tumor
c) incidence of oral lesion in AIDS 50%
d) predisposing factors ???
e) treat with intralesion vinca alkyloids or interferon
- thrombocytopenia
a) blood platelets < 100,000/ cc
b) marrow suppression due to infection, leukemic infiltrate, aplastic
anemia
- seborrheic keratosis
a) middle aged to elderly
b) head, neck, trunk
c) sharply demarcated plaques with rough surface
d) in African Americans, dermatosis papulosa nigra 35% incidence
21. Depigmented Lesions
- vitiligo
a) autoimmune destruction of melanocytes
b) autoantibody to melanocytes formed inkeratinocytes
c) scalp lesions common
- albinism
a) melanocytes are inactive but not destroyed
22. Yellow and Orange Lesions
- Fordyce granules
a) multiple small elevated asymptomatic papules
b) ectopic sebaceous glands
c) buccal mucosa most common location
d) increase at puberty
- parulis
a) dento-alveolar abscess with purulent drainage
b) may be painful until drainage occurs
c) strep, staph, actinomyces
- lymphoepithelial inclusion cyst
a) lymph appears yellow clinically
b) embryologically entrapped epithelium in lymphoid aggregates
c) superficial floor of mouth location common
d) conservative excision
- lipoma
a) common to skin, uncommon to mucosa
b) tongue, buccal mucosa, labial mucosa most common sites
- lymphonodular pharyngitis
a) multiple aggregates in Waldheyer’s ring area
b) coxsackle A10 virus
c) 5 day incubation followed by sore throat, fever, headache
d) 2 week course
e) supportive therapy
- jaundice
a) secondary to organ dysfunction or drug therapy
* viral hepatitis
* sickle cell or hemolytic anemia
* congestive heart failure
* renal failure
* hepatocellular carcinoma or metastatic tumor to liver
* quinacrine therapy
b) liver metabolism of hemoglobin breakdown to bilirubin
* liver capacity to metabolize bilirubin 2.0 mg/dl
* unconjugated bilirubin brought to liver bound to albumin
* liver conjugates to water soluble form for excretion in bile
c) excess rbc breakdown overwhelms hepatic capacity in hemolytic
anemia
d) hepatitis and cirrhosis prevent conjugation to water soluble state
e) obstruction by tumor or gallstones prevents excretion of bile once
conjugated
- Tangier’s disease
a) hereditary high density lipoprotein deficiency
b) Tangier’s island inhabitants - consanguinity allows autosomal
recessive trait to be expressed
c) gingival enlargement and deposition of cholesterol in tonsillar
tissue producing orange discoloration
d) loss of protective effect from high density lipoprotein results in
higher than expected incidence of atherosclerosis and arteriosclerosis
Tidak ada komentar:
Posting Komentar