“Definition of Impacted tooth”
An impacted tooth is any tooth that is prevented from reaching its normal position in the mouth by tissue, bone, or another tooth.
Of the surgical procedures performed in the oral cavity, the removal of impacted and semi-impacted teeth is the most common. The extraction of these teeth, depending on their localization, may prove to be relatively easy or extremely difficult and laborious. Regardless of the degree of difficulty of the surgical procedure though, its success primarily depends on correct preoperative evaluation and planning, as well as on the treatment of complications that may arise during the procedure, or the management of complications that may present after the surgical procedure. For these reasons, a medical history, clinical examination of the patient, and radiographic evaluation of the area surrounding the impacted tooth are deemed necessary.
Indications for removal of impacted tooth
Specialists have divergent points of view concerning the necessity to extract impacted teeth. Certain people suggest that the removal of impacted teeth is necessary as soon as their presence is confirmed, which is usually by chance. They even believe that it must be done as soon as possible, as long as there is no possibility that the impacted tooth may be brought into alignment in the dental arch using a combination of orthodontic and surgical techniques. On the other hand, others suggest that the preventive removal of asymptomatic impacted teeth, besides subjecting the patient to undue discomfort, entails the risk of causing serious local complications (e.g., nerve damage, displacement of the tooth into the maxillary sinus, fracture of the maxillary tuberosity, loss of support of adjacent teeth, etc.). As far as impacted teeth that have already caused problems are concerned,everyone agrees that they should be removed, regardless of the degree of difficulty of the surgical procedure. The most common of these problems are now given.

Pericoronitis in a semi-impacted mandibular third molar. Diagrammatic illustration showing inflammation under the operculum and distal to the crown of the tooth.

Clinical photograph. Characteristic swelling of the operculum due to constant biting from the antagonist
Localized or Generalized Neuralgias of the Head(Prevention of pain of unexplained origin.
Impacted teeth may be responsible for a variety of symptoms related to headaches and various types of neuralgias. If this is the case, the pain may be due to pressure exerted by the impacted tooth where it comes into contact with many nerve endings. Many people suggest that the symptoms may subside after the removal of the offending tooth, which basically involves ectopic impacted teeth.
Pericoronitis.
This is an acute infection of the soft tissues covering the semi-impacted tooth and the associated follicle. This condition may be due to injury of the operculum (soft tissues covering the tooth) by the antagonist third molar or because of entrapment of food under the operculum, resulting in bacterial invasion and infection of the area. After inflammation occurs, it remains permanent and causes acute episodes from time to time. It presents as severe pain in the region of the affected tooth,which radiates to the ear, temporomandibular joint, and posterior submandibular region. Trismus, difficulty in swallowing, submandibular lymphadenitis, rubor, and edema of the operculum are also noted. A characteristic of pericoronitis is that when pressure is applied to the operculum, severe pain and discharge of pus are observed. Acute pericoronitis is often responsible for the spread of infection to various regions of the neck and facial area.
Production of Caries.
Entrapment of food particles and bad hygiene, due to the presence of the semi-impacted tooth, may cause caries at the distal surface of the second molar, as well as on the crown of the impacted tooth itself.
Decreased Bone Support of Second Molar.
The well-timed extraction of a semi-impacted tooth presenting a periodontal pocket ensures the avoidance of resorption of the distal bone aspect of the second molar, which would result in a decrease of its support.
Obstruction of Placement of a Partial or Complete Denture.
The impacted teeth of edentulous patients can erupt towards the residual alveolar ridge, creating problems when applying a prosthesis. The localization of the tooth is often observed after its communication with the oral cavity and the presence of pain and edema.
Obstruction of the Normal Eruption of Permanent Teeth.
Impacted teeth and supernumerary teeth often hinder the normal eruption of permanent teeth, creating functional and esthetic problems.
Provoking or Aggravating Orthodontic Problems.
Lack of roomin the arch is possibly themost common indication for extraction, primarily of impacted and semi-impacted third molars of the maxilla and mandible.
Participation in the Development of Various Pathologic Conditions.
The coexistence of an impacted tooth and various pathologic conditions is not an uncommon phenomenon. Often cystic lesions develop around the crown of the tooth and are depicted on the radiograph as different-sized radiolucencies. These cysts may be large and may displace the impacted tooth to any position in the jaw. Whenthe presence of such osteolytic lesions is verified radiographically, they must be removed together with the associated impacted tooth.
Destruction of Adjacent Teeth Due to Resorption of Roots.
Resorption of the roots of adjacent teeth is another undesirable situation that may be caused by the impacted tooth; the effect isbrought about through pressure. This case primarily involves the posterior teeth of the maxilla and mandible. It begins with resorption of the distal root and, eventually, may totally destroy the tooth. The resorption of rootsmay also be observed in other areas of the dental arch and may involve dental surfaces other than those mentioned above. Having mentioned the undesirable situations that are associated with impacted teeth, and given the fact that no one can guarantee that an asymptomatic impacted tooth will not create problems in the future, the choice of removing or preserving the impacted tooth must be made after considering all the possibilities.
Prevention of fracture of jaws
Prevention of Periodontal Disease
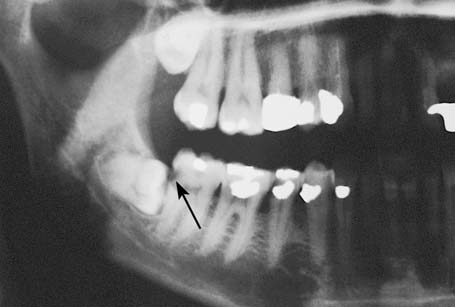
Caries on the distal surface of the second molar, caused by a semi-impacted mandibular thirdmolar

Caries in the distal area of the crown of semi impacted third molar, due to entrapment of food and bad hygiene

Bone resorption at the distal surface of the root of a mandibular second molar, resulting in a periodontal pocket

Impacted mandibular third molar in edentulous area, which erupted after placement of a partial denture

Obstruction of the eruption of a mandibular second molar because of an impacted third molar

Impacted maxillary central incisor, whose eruption was obstructed because of a supernumerary tooth

Impacted mandibular third molar with well-defined radiolucency at the distal area

Impacted mandibular canine that is surrounded by a lesion

Extensive radiolucent lesion in the posterior area of the mandible, occupying the ramus. The impacted tooth has been displaced to the inferior border of the mandible.

Extensive radiolucent lesion in the mandible, extending from the mandibular notch as far as the canine. The impacted tooth has been displaced to an area high in the ramus of the mandible

Complete resorption of the distal root of the left mandibular firstmolar, due to an impacted second molar
Medical History
A detailed medical history is necessary because, based on the information provided, useful information may be found concerning the general health of the patient to be operated on. This information determines the preoperative preparation of the patient, as well as the postoperative care instructions.
Clinical Examination
During the intraoral clinical examination, the degree of difficulty of access to the tooth is determined, especially concerning impacted third molars. When the patient cannot open his or her mouth, because of trismus that is mainly due to inflammation, the trismus is treated first, and extraction of the third molar is performed at a later date. In certain cases of impacted teeth, especially canines, buccal or palatal protuberance may be observed during palpation or even inspection, which suggests that the impacted tooth is located underneath. Also, the adjacent teeth are examined and inspected (extensive caries, large amalgam restorations, prosthetic appliance, etc.) to ensure their integrity during manipulations with various instruments during the extraction procedure.
Radiographic Examination
The radiographic examination provides us with all the necessary information to program and correctly plan the surgical removal of impacted teeth. This information includes: position and type of impaction, relationship of impacted tooth to adjacent teeth, size and shape of impacted tooth, depth of impaction in bone, density of bone surrounding impacted tooth, and the relationship of the impacted tooth to various anatomic structures, such as the mandibular canal, mental foramen, and the maxillary sinus. These aforementioned data may also be provided by periapical radiographs and panoramic radiographs, as well as occlusal radiographs.
Assessment and Classification of Impacted third molar
Impacted Third Molar Classification.
The impacted mandibular third molar may present with various positions in the bone, and so the technique for its removal is determined by its localization. The classic positions of the tooth, depending on the direction of the crown of the tooth, are (according to Archer 1975; Kruger 1984): mesioangular, distoangular, vertical, horizontal, buccoangular, linguoangular, and inverted. Impacted teeth may also be classified according to their depth of impaction, their proximity to the second molar, as well as their localization in terms of the distance between the distal aspect of the second molar and the anterior border of the ramus of themandible. As far as the depth of impaction is concerned, mandibular third molars may be classified (according to Pell and Gregory 1933) as belonging to three categories:
Class A: The occlusal surface of the impacted tooth is at the same level as, or a little below that of, the second molar.
Class B: The occlusal surface of the impacted tooth is at the middle of the crown of the second molar or at the same level as the cervical line.
Class C: The occlusal surface of the impacted tooth is below the cervical line of the second molar As for the distance to the anterior border of the ramus of the mandible, impacted teeth may be classified as belonging to one of the following three categories:

Classification of impaction of mandibular third molars, according to Archer (1975) and Kruger (1984). (1Mesioangular, 2 distoangular, 3 vertical, 4 horizontal, 5 buccoangular, 6 linguoangular, 7 inverted)
Class 1: The distance between the second molar and the anterior border of the ramus is greater than the mesio distal diameter of the crown of the impacted tooth, so that its extraction does not require bone removal from the region of the ramus.
Class 2: The distance is less and the existing space is less than the mesiodistal diameter of the crown of the impacted tooth.
Class 3: There is no room between the second molar and the anterior border of the ramus, so that the entire impacted tooth or part of it is embedded in the ramus.

Classification of impacted mandibular third molars according to Pell and Gregory (1933): a according to the depth of impaction and proximity to the second molar; b their position according to the distance between the secondmolar and the anterior border of the ramus of the mandible
The above classification methods refer to all of the aforementioned positions of the impacted tooth. Furthermore, the number of roots of the impacted tooth and their relationship to the mandibular canal are taken into consideration. It is obvious that the cases belonging to Class 3 present more difficulty during the surgical procedure, because the extraction of the tooth requires removal of a relatively large amount of bone and there is a risk of fracturing the mandible and damaging the inferior alveolar nerve.
Winter's Lines (WAR)
The position & depth of the mandibular 3rd molar can be determined using the Winter’s Lines (WAR). These are 3 imaginary lines (red, amber & white) “drawn” on the dental X-ray (these days, normally an OPG / DPT).
The position & depth of the mandibular 3rd molar can be determined using the Winter’s Lines (WAR). These are 3 imaginary lines (red, amber & white) “drawn” on the dental X-ray (these days, normally an OPG / DPT).

White Line
The white line is drawn along the occlusal surfaces of the erupted mandibular molars & extended over the 3rd molar posteriorly. It indicates the difference in occlusal level of the 1st & 2nd molars & the 3rd molar.
Amber Line
The amber line represents the (height of the) bone level. The amber line is drawn from the surface of the bone on the distal aspect of the 3rd molar (or from the ascending ramus) to the crest of the inter dental septum twixt the 1st & 2nd molars. This line denotes the margin of the alveolar bone covering the 3rd molar and gives some indication to the amount of bone that will need to be removed for the
tooth to come out.
Red Line
The red line is an imaginary line drawn perpendicular from the amber line to an imaginary point of application of an elevator. Usually, this is the cemento-enamel junction on the mesial aspect of the impacted tooth (unless, it is the disto-angular impacted tooth where the application point is the distal cemento-enamel junction). The red line indicates the amount of bone that will have to be removed before elevation of the tooth i.e. the depth of the tooth in the jaw & the difficulty encountered in removing the tooth.
With each increase in length of the red line by 1mm, the impacted tooth becomes 3 x more difficult to remove (as opined by Howe). If the red line is < 5mm, than the tooth can be removed under just LA; anything above, a GA or LA Sedation would be more appropriate.
Another method of judging the depth of the 3rd molar is to divide the root of the 2nd molar into thirds. A horizontal line is drawn from the point of application for an elevator to the 2nd molar. If the point of application is adjacent to the coronal, middle or apical root third, then the tooth extraction is assessed as easy, moderate or difficult respectively.

Steps of Surgical Procedure
The surgical procedure for the extraction of impacted teeth includes the following steps:
1. Incision and reflection of the mucoperiosteal flap
2. Removal of bone to expose the impacted tooth
3. Luxation of the tooth
4. Care of the postsurgical socket and suturing of the wound
The main factors for a successful outcome to the surgical procedure are as follows:
· Correct flap design, which must be based on the clinical and radiographic examination (position of tooth, relationship of roots to anatomic structures, root morphology).
· Ensuring the pathway for removal of the impacted tooth, with as little bone removal as possible. This is achieved when the tooth is sectioned and removed in segments, which causes the least trauma possible.
Principles of Mucoperiosteal flap design
1. Preservation of blood supply
2. Adequate access
3. Prevent damage to vital structures
4. Incision margins should lie on sound bony margins
5. Ease of repositioning
Types of Flaps.
According to the type of incision
· Envelope
· Two sided
· Three sided
· Apically repositioned flap
· Semilunar
According to the thickness
· Full thickness
· Partial thickness
According to the site
· Labial or buccal flap
· Palatal or Lingual flap
Many types of flaps may be used when surgically removing impacted mandibular third molars: the triangular and the envelope flap are the commonest using flaps. The choice depends on the evaluation of the various data pertaining to the case (e.g., depth of impaction, position, etc.).
Triangular flap:
The incision for this type of flap begins at the anterior border of the ramus (external oblique ridge) with special care for the lingual nerve and extends as far as the distal aspect of the second molar, while the vertical releasing incision is made obliquely downwards and forward, ending in the vestibular fold In certain cases, e.g., when impaction is deep, to ensure a satisfactory surgical field or when the impacted tooth conceals the roots of the second molar, the incision may continue along the cervical line of the last tooth while the vertical incision begins at the distal aspect of the first molar.


Variation of incision shown in figure (vertical releasing incision is distal to the first molar). The mesial extension of incision is necessary due to the position of the third molar compared to the second molar
Horizontal (envelope) flap:
The incision for the flap also begins at the anterior border of the ramus and extends as far as the distal aspect of the second molar, continuing along the cervical lines of the last two teeth, and ending at the mesial aspect of the first molar. This type of flap is usually used in cases where impaction is relatively superficial.


Clinical photograph and b diagrammatic illustration showing incision for envelope flap
Anesthesia.
Anesthesia in cases of impacted mandibular third molars is achieved by: inferior alveolar nerve block, buccal nerve block, lingual nerve block, and local infiltration for hemostasis in the surgical field.
Techniques of bone removal
· Use of Burs
· Use of chisel and mallet
Bone removal with burs-Points to remember
· Copius irrigation
· Protect vital structures
Principles of closure of flaps
· Gentle tissue handling
· Not too tight sutures
· Haemostasis prior to closing
· Avoid dead space
· Decontamination and debridement
· Proper approximation
Surgical removal of different types of impactions will be discussed in later posts
Tidak ada komentar:
Posting Komentar